Achalasia is a disorder of the esophagus that makes it difficult for foods
and liquids to pass into the stomach. This process typically progresses
over time with increasing esophageal enlargement despite therapy. A Heller
Myotomy is a procedure in which the lower esophageal muscles are cut to
help open the abnormally tight valve between the esophagus and the stomach.
This helps to relieve dysphagia (difficulty swallowing).
Procedure Overview
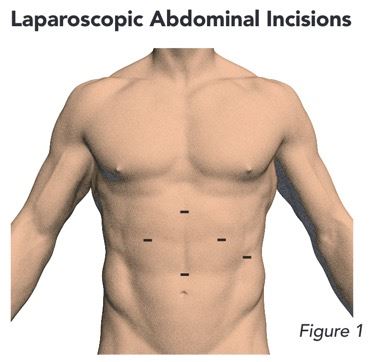
Heller Myotomy is performed under general anesthesia, so you will be asleep
throughout the entire procedure. It is performed through 5 to 6 small
incisions in your abdomen.
(Figure 1) The surgery can take approximately 2 to 4 hours.
In-Hospital Recovery
Pain Management: A multi-modal pain regimen is used along with narcotic pain medications.
You will receive three medications prior to surgery, while in the hospital
and upon discharge home to help control your pain postoperatively. These
are: Tylenol, Gabapentin, and Celebrex or ibuprofen. Depending on your
age, you will also be given an anti-nausea patch called Scopolamine.
A stronger pain medication may be given, to include a narcotic, for any
breakthrough pain.
Diet: You will be allowed a clear liquid diet within the first 24 hours of your
surgery. Sips of water to take medication will be allowed. On the day
following your procedure, you will have a special test performed (barium
esophagram) in which you will be asked to swallow contrast and x-rays
will be taken. If this study is acceptable and no leak is shown, you will
be advanced to a liquid diet. You will most likely be discharged at this
point and given specific instructions on what diet to follow upon returning home.
Recovery at Home
Pain: As stated above, you will be given prescriptions and specific instructions
for a pain control regimen. These medications include Tylenol, Gabapentin,
Celebrex or ibruprofen, and possibly a stronger pain medication for breakthrough pain.
Activity: After discharge, your activity level should increase gradually over time.
You should avoid heavy lifting for an INDEFINITE amount of time following
surgery, and this will be reviewed with you after surgery. Avoid lifting
anything heavier than 20-25 lbs. Most patients can return to work in 1
to 2 weeks depending on their occupation.
Driving: You should avoid driving for at least 5 days following surgery. You are
not cleared to drive until you are no longer taking narcotic pain medication.
Wound Care: Your incision sites will be covered with purple-colored surgical glue
called Dermabond. This glue will come off on its own with time. You may
shower normally after surgery, pat-do not rub-your incision sites and
leave them open to air. Do not soak in a bathtub or swim in a pool for
at least 4-6 weeks following your surgery.
Pre-Operative Testing
A series of tests may be performed to determine if you are a candidate
for esophageal surgery. These include upper endoscopy, barium swallow
test, ambulatory pH test, and esophageal manometry.
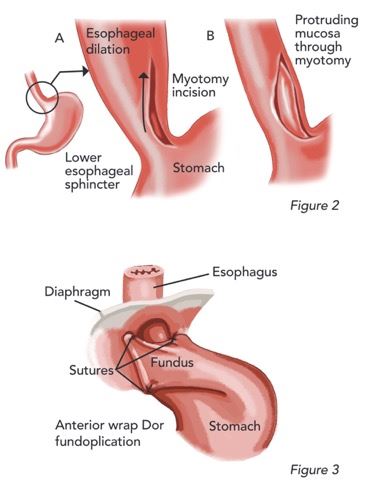
New Anatomy
During your procedure, the muscles that cover the lower esophagus and valve
that connects the esophagus to the stomach are cut to help open this area.
This is called a myotomy.
(Figure 2) Some patients experience worsening reflux following this procedure and
therefore a partial anterior fundoplication (Dor fundoplication) will
be performed to decrease the likelihood of this occurring. A partial fundoplication
is when the top part of the stomach, or the fundus, is wrapped over top
of the end of the esophagus and tied down with special suture.
(Figure 3)
Surgical Results
Most patients have good outcomes with surgical myotomy, with better outcomes
compared to non-surgical treatment, although 10%-30% of patients will
experience recurrence within 10 years of surgery. Recent studies show
that almost all patients will have to undergo some other type of intervention
during their lifetime.

 Cardiac Surgery, Cardiothoracic SurgeryView Profile
Cardiac Surgery, Cardiothoracic SurgeryView Profile









