Definition: An esophagectomy is a surgical procedure that removes part of the diseased
esophagus (tube between your mouth and stomach) and reconstructs it using
part of another organ, typically the stomach. This type of procedure is
typically used for esophageal cancer. While this procedure may be completed
in many ways, a minimally invasive approach is always the first consideration.
Esophagectomy is the cornerstone of multidisciplinary therapy for patients
with localized disease, or disease confined to the esophagus. About 22%
of patients diagnosed with esophageal cancer have localized disease.
Prior to surgery, some patients will require chemotherapy, radiation therapy,
or a combination of both. Treatment given prior to surgery is called neoadjuvant
therapy. The decision to give neoadjuvant therapy is based on the clinical
stage of your cancer. Your surgeon and oncologist will discuss this with
you during your consultation.
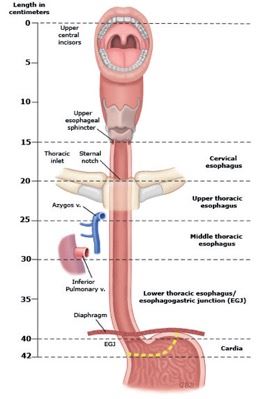
Figure 1 below demonstrates the different regions and anatomy of the esophagus.
Your tumor may be in the cervical region, upper thoracic esophagus, middle
thoracic esophagus, or lower thoracic esophagus.
AJCC 8th Edition Regions of the Esophagus
Figure 1 Modified Image from Rice, TW, Kelsen D, Blackstone EH, et al.
Esophagus and esophagogastric junction. In: AJCC Cancer Staging Manual,
8th Ed, Amin MB (ed), Springer Science+Business Media, LLC, New York, 2017.
Surgical Approach:
Within this section, the different approaches to an esophagectomy are discussed.
Please keep in mind that each surgical approach depends on the patient.
Your surgeon will discuss this with you in detail prior to your scheduled
procedure.
Three-Incision Esophagectomy:
The three-incision esophagectomy refers to the three access points that
the surgeon will use to complete the procedure. The first area is the
right chest. When possible, this is done in a minimally invasive approach
known as a Video-Assisted or Robotic-Assisted Thoracoscopic Surgery. During
this approach, small incisions, 1 to 4 cm in length, are made on your
right chest. A camera is used to help the surgeon see your internal anatomy.
The other incision sites are used to insert special instruments that are
needed to complete your surgery (Figure 2).
The abdomen is the next part of your body that will need to be accessed.
This is attempted using a minimally invasive approach, with 5 to 6 small
incisions (Figure 3). Again, a camera is placed through one of these sites
and used to look directly at your internal organs. Following the laparoscopic
portion of the operation, an open incision from the sternum to the navel
may be made so that your surgeon can access your stomach in preparation
for the creation of the gastric conduit (the portion of your stomach that
will replace the diseased portion of your esophagus) (Figure 4).
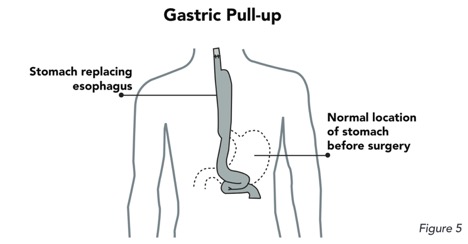
The last incision is made on the left side of the neck. This incision allows
your surgeon to attach the healthy esophagus and new gastric conduit (the
portion of the stomach that replaces the diseased portion of your esophagus).
Your surgeon will use a variety of stitches and stapling devices to make
sure the connection between the two structures is secure. (Figure 5).
Preparation for Surgery
You will be required to have a series of tests prior to your scheduled
procedure. These tests include a breathing test (pulmonary function testing),
a cardiac stress test, echocardiogram, EKG (heart tracing), and blood work.
You will not be able to eat starting at midnight the night before your
operation. You may have clear liquids, such as water or black coffee,
up until 2 hours prior to your procedure. You will be given a pamphlet
with more details about this. If you take medications routinely at home,
we will discuss which of these you can take before your operation.
After you have been placed under general anesthesia, a catheter is inserted
into your bladder to monitor your urine output during and after surgery.
Pain management is achieved with a combination of intravenous and oral
pain medications. The surgeon will also place a nerve block in the chest
wall area that ideally lasts for three days after surgery. You will be
transitioned to pain medication by mouth as you prepare for discharge
from the hospital.
After your Surgery
Your operation will typically take anywhere from 6 to 10 hours. After your
surgery has been completed, you will recover in the intensive care unit
(ICU) where the nursing staff will monitor you closely around the clock.
Most patients are brought into the ICU from the operating room with a
breathing tube still in place. This breathing tube is typically removed
the night of surgery or the following morning. You should expect to have
a tube down your nose that goes into your stomach, 1 to 2 chest tubes
on the right side of your chest, a small drain from the incision on the
left side of your neck, a urinary catheter, and a feeding tube. You will
remain in the ICU usually overnight following your surgery, depending
on your recovery process. Once you are stable and ready to be transferred
out of the ICU, you will be taken to the step-down unit, 2 South. Patients
are typically stable enough to go home within 7 to 10 days following surgery.
You will go home with your feeding tube in place; all other lines and
tubes will be removed before you leave the hospital.
Diet: You will not be able to take anything by mouth for the first 4 to 5 days
following your surgery. Nutrition will be given through your feeding tube
during this time to help you stay strong during recovery. You will undergo
a study called an esophagram about 5 days after your surgery. During this
study, you will swallow contrast and x-rays will be taken. This test looks
to see if the connection between the healthy esophagus and new gastric
conduit (the portion of the stomach that replaces the diseased portion
of your esophagus) is healing properly. If the study shows no leak, you
will be able to start a clear liquid diet. Your diet will gradually progress
to include all liquids. Upon discharge, we will review the diet you are
to follow. Your diet upon discharge is dependent on your progress while
in the hospital and will be decided by your surgeon. You may also be required
to continue tube feedings at home. We will have a nutritionist consult with you.
References:
1. Figure 1: AJCC: American Joint Committee on Cancer; v: vein.
Modified from: Rice, TW, Kelsen D, Blackstone EH, et al. Esophagus and
esophagogastric junction. In: AJCC Cancer Staging Manual, 8th Ed, Amin
MB (ed), Springer Science+Business Media, LLC, New York, 2017. Graphic 111260 Version 5.0

 Within this section, the different approaches to an esophagectomy are discussed.
Please keep in mind that each surgical approach depends on the patient.
Your surgeon will discuss this with you in detail prior to your scheduled
procedure.
Within this section, the different approaches to an esophagectomy are discussed.
Please keep in mind that each surgical approach depends on the patient.
Your surgeon will discuss this with you in detail prior to your scheduled
procedure.
 Cardiac Surgery, Cardiothoracic SurgeryView Profile
Cardiac Surgery, Cardiothoracic SurgeryView Profile









