A lung resection is the removal of a part or entire lobe of your lung.
There are different ways that a lung resection surgery can be performed.
These will be discussed below.
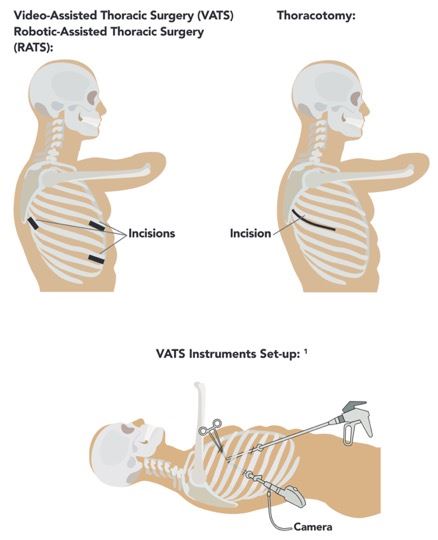
There are three different approaches that your surgeon can use to remove
part of your lung: VATS, RATS, and thoracotomy. VATS stands for Video-Assisted
Thoracoscopic Surgery. RATS stands for Robotic-Assisted Thoracoscopic
Surgery. A thoracotomy is a larger incision made between the ribs, requiring
rib spreading. A VATS and RATS approach are both considered to be minimally
invasive with small incision sites made. Your surgeon will discuss with
you which of the above approaches is best for you. This operation is done
under a general anesthesia and typically takes between 2 to 4 hours. After
you are asleep, you will be positioned on your side. During a VATS or
RATS approach, your surgeon will make small incisions on the side of your
chest that are about 1 to 4 cm in length. One of these incision sites
is used for a camera to look around inside of your chest. The other incision
sites are used for special instruments that are used to perform the operation.
A special stapling device is used during the operation to remove lung
tissue, divide blood vessels, and divide the bronchus (airway that is
supplying your lung). Lymph node samples are typically removed during
this procedure. The key element of VATS/RATS approach is to avoid spreading
of the ribs.
At the end of the operation, the incision sites that were made will be
closed using absorbable stitches that are underneath the skin. Typically,
one or two of those incision sites will be used for a chest tube which
drains any air or fluid that may still be in the chest after the operation.
You will typically wake up with 1 to 2 chest tubes in place following
the operation. Any lung tissue and lymph node samples that were removed
during the operation will be sent to the laboratory for analysis, with
results typically returned in about a week.
Your Operation: Surgical Approach
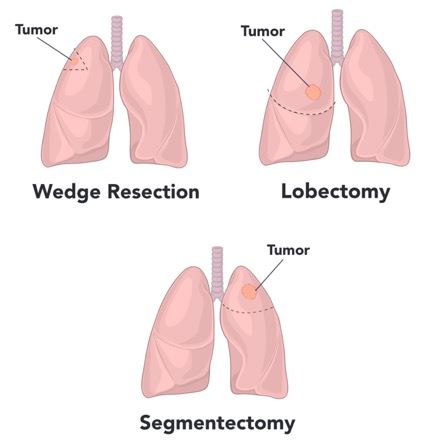
What are the Different Types of Lung Resections?
There are a few different types of lung resection procedures. Below we
will discuss the differences between a wedge resection, lobectomy and
segmentectomy.
Wedge Resection:
A wedge resection is a procedure that involves the surgical removal of
a small, wedge-shaped piece of lung tissue. This can be used to remove
or diagnose a small tumor or to diagnose different types of lung disease.
This type of procedure is not ideal for treatment of lung cancer although
it is sometimes preferred for patients who cannot tolerate the removal
of a large section of lung when there may be a significant decrease in
lung function. Your surgeon will discuss the reasons to undergo a wedge
resection with you in detail prior to your procedure. 3.
Anatomic Lung Resection: Lobectomy and Segmentectomy:
Lobectomy: A lobectomy is a surgical procedure where an entire lobe of your lung is
removed for a variety of reasons, but most commonly for treatment of lung
cancer. There are three lobes that make up your right lung (right upper
lobe, right middle lobe, right lower lobe) and two lobes that make up
your left lung (left upper lobe, left lower lobe). During this type of
lung resection, blood supply to the specific lung lobe that is being removed
does need to be closed off. The bronchus is a tube-like structure that
supplies air to your lungs. This structure also needs to be closed off
prior to the removal of the lung lobe. The above is done using a special
type of stapler that will securely divide these structures. 4
Segmentectomy: A segmentectomy is a lung resection that involves the removal of part
of one of the lobes of the lung. As stated above, the right lung is divided
into three lobes and the left lung is divided into two lobes. These lobes
are subdivided into segments. This type of resection spares more lung
tissue as compared to a lobectomy, therefore leaving a patient with higher
lung reserve. In certain circumstances, you may be a candidate for a segmental
lung resection. Your surgeon will have this discussion with you and decide
which type of lung resection is right for you.
Understanding your Operation
If you are having a section of your lung removed, there are different approaches
that your surgeon can do to remove part of your lung. The approach depends
on the location and extent of your disease as well as your overall health.
Changes to Planned Surgery
There is always a risk that your surgery may not be able to be completed
as planned. Sometimes the surgeon may be unable to do your operation using
the VATS/RATS approach and therefore must extend one of the incision sites
to make a longer cut to enable the completion of the operation; this is
called a thoracotomy. Very rarely, if there is bleeding during the operation
that cannot be controlled through the VATS/RATS incisions, the surgeon
will need to make a longer cut to gain direct vision and control the bleeding.
In addition, sometimes unexpected findings may change the plan for the surgery.
Preparation for Surgery
Most importantly, if you currently smoke, we strongly recommend that you
stop at least three weeks prior to your scheduled procedure. Your risk
of post-operative complications is drastically increased if you continue
to smoke up until the day of your surgery. You will be asked to start
a daily walking program prior to your surgery. This will be discussed
in detail with you by your surgeon. You will most likely be required to
have some testing completed prior to your lung resection surgery. Some
of these tests include a breathing test (pulmonary function test), EKG
(heart tracing), cardiac stress test, echocardiogram and blood work. You
will not be able to have anything to eat starting at midnight the night
before your operation. You can have clear liquids, such as water or black
coffee, up until 2 hours prior to your procedure. You will be given a
pamphlet with more details regarding this. If you take medications routinely
at home, we will discuss which of these you can take before your operation
and which you cannot. Prior to your surgery after you have been put to
sleep, a catheter will be inserted into your bladder to monitor your urine
output during and after the surgery. 6
After your Surgery
After your surgery has been completed, you will be taken to the recovery
room. The nursing staff will monitor your vital signs (blood pressure,
breathing rate, oxygen levels, heart rate) and make sure that you are
comfortable. You will wake up with 1 to 2 chest tubes in place. You will
remain in recovery for about 2 hours after your procedure and then you
will be taken to your hospital room in the step down unit (2 south). You
will be given supplemental oxygen to help you breath. You will also be
receiving fluids through your IV. You will be able to drink and eat as
soon as you can tolerate. The urinary catheter is typically removed the
morning after surgery. The chest tubes will remain in place for at least
24 to 48 hours depending on the amount of drainage and if there are any
air leaks present; this is determined by your surgeon. You will be getting
many chest x-rays while you are in the hospital, so expect to be awoken
early in the morning for this to be completed. You will be instructed
on breathing exercises and deep coughing to prevent any chest infections.
You will also be encouraged to walk in the hallway and exercise your legs
to prevent any blood clots from forming. Walking is very important and
you will be encouraged to get out of bed the same day as your surgery.
Pain Control: Following your procedure you should expect to have pain. We will control
your pain with a multi-modal regimen including Tylenol, Gabapentin (helps
nerve pain), and Celebrex (anti-inflammatory). You will also be given
a narcotic pain medication as needed. We try to keep IV pain medication
to a minimum, but each patient is different and pain medications will
be adjusted as needed.
General Care: You will be expected to start walking either the night of surgery or the
day following. The dressings over your chest tube site will be removed
following removal of the chest tubes. The other incision site dressings
will be removed in the office at your follow-up appointment. Once your
chest tubes are removed, you are able to shower daily and are encouraged
to do so. Patients are typically ready to be discharged home 2-4 days
after their procedure.
Risks and Possible Complications
With any surgical procedure, there are certain risks associated and these
risks will depend on your health before undergoing the operation. Your
surgeon will discuss these risks with you in detail.
Sore throat: It is normal to have a sore throat following surgery. It is a result of
being under anesthesia and having a breathing tube during the operation.
This should get better shortly after surgery.
Changes in blood pressure/heart rate: Sometimes your blood pressure may be lower/higher after having anesthesia.
This is normally due to not having anything to eat or drink prior to surgery
and the medications you receive in the operating room. Your blood pressure
may normalize once you begin having fluid intake. Your heart rate may
be disrupted as well during the procedure. You will be given a medication,
Metoprolol, in the hospital and at discharge to prevent any irregular
heart rhythms or rates.
Coughing up blood (Hemoptysis): It is normal to cough up small amounts of blood tinged sputum (usually
the size of a quarter) for the first few days after lung resection surgery.
This will gradually reduce with time.
Chest infection/Pneumonia: Breathing exercises, walking, getting out of bed and adequate pain control
will reduce the risk of a chest infection. Your chance of chest infection
or pneumonia is 8 times more likely if you are a current smoker. If you
do develop a chest infection, you may need treatment with an antibiotic
and your hospital stay may be longer.
Air leaks: This is when the cut surface of the lung tissue leaks air. This typically
resolves on its own in a few days however it does mean that your chest
tubes will have to stay in place while it heals. Sometimes this means
you will be sent home with a chest tube in place.
Pneumothorax: Occasionally the lung will not fully inflate following surgery and this
may require having a chest tube in place for a longer duration. Sometimes
this can occur after the chest tube is removed. In these instances, another
chest tube may have to be placed to allow the lung to fully re-expand.
Heart attack or stroke: This can occur during or after any surgery. The risk is higher in patients
with a cardiac history or undiagnosed cardiac disease. For this reason,
every patient will have cardiac work-up completed prior to your procedure.
Discharge
Your follow-up will be scheduled prior to you leaving the hospital. You
will be seeing an advanced practice provider at your initial post-operative
visit. You will be asked to get a chest x-ray completed at Medical Imaging
of Fredericksburg prior to your appointment (that same day).
References:
1. VATS Instruments:
Diagram showing video assisted thoracoscopy.
2. RATS Set-up Picture:
Robotic Approach to Lobectomy. Thoracic Key.

 Cardiac Surgery, Cardiothoracic SurgeryView Profile
Cardiac Surgery, Cardiothoracic SurgeryView Profile









